[All three Shrink Rappers have contributed to this post] 
There's an article over at
PLoS Medicine about antidepressants that makes for interesting reading. The article,
Antidepressants and Violence: Problems at the Interface of Medicine and Law by David Healy, Andrew Herxheimer, & David B. Menkes, reviews pharmaceutical company data regarding
SSRI-induced violence, aggression, and hostility. The main antidepressant reviewed is paroxetine (Paxil, Seroxat, others), though fluoxetine/Prozac, sertraline/Zoloft, and venlafaxine/Effexor XR, are mentioned.
The three authors acknowledge that they have all served as expert witnesses supporting and opposing the role of SSRI antidepressants, which makes the article seem a bit like an advertisement for their expert witness business. Nonetheless, the review of drug company data (mostly GSK) is worth a gander.
Roy: I found most interesting the low incidence of episodes of "hostility" among both those on drug or placebo. For example there were only 55 (0.4%) reports of "aggression" or "assault" in 13,741
adverse effect monitoring reports from the UK of paroxetine, and 1 report of "murder". I'll leave it to the reader to find incidence reports in the general population, but I'm guessing it is at least this or higher.
GlaxoSmithKline's
data from
all of their placebo-controlled paroxetine trials showed "hostility events" (which includes mere thoughts as well as actions) in a total of 60 out 9219 paroxetine cases (0.65%) and 20 out of 6455 placebo cases (0.31%). Statistically, one appears to be twice as likely to have an "hostility event" on Paxil than on placebo.
The lawyers are lining up at the courthouse for business (Clink, feel free to pick up on that one).
The article, which anyone can view in its entirety (that's what I like about PLoS Journals), includes 9 actual case examples or folks who did bad things, like robbery and murder, after taking SSRIs (sometimes after only 2 doses).
Clink:
There's a reason why this article was not published in a standard peer-reviewed journal. It seems like an article that can't make up it's mind about what to discuss. It didn't really address the legal issues involved in drug-related criminal prosecution and it's an incomplete discussion of the clinical studies. Frankly, I left the article feeling a little bothered by the lack of focus.
Regarding the clinical issues: violence is a multifactorial behavior, and I think it's overly simplistic to reduce it to a simple medication cause-and-effect. Confounding variables are the presence of personality disorders, previous acts of violence, active affective disorder symptoms and co-existing substance abuse. We know nothing about these confounding variables from this article. While clinical trial data will be useful to identify strong associations that could be attributed to medications (eg. weight gain, increases in prolactin levels) it is less useful for low base-rate phenomena like homicide. As Roy has already pointed out, base rates of general aggression were low to begin with in the clinical monitoring data from the UK.
Regarding the legal issues: that was actually the interesting part for me, and they totally glossed over it! They only presented their own small case series. They didn't discuss diminished capacity defenses, insanity or involuntary intoxication. To keep it simple (and to minimize the length of this post) I'm only going to talk about involuntary intoxication.
When it comes to mental health defenses in crime, all jurisdictions exclude voluntary intoxication as a defense. This is done for the obvious reason that the majority of violent offenses occur under the influence of drugs and alcohol, so social policy dictates that people must be held accountable for the consequences of their choice to abuse substances. However, longterm use of some substances can cause permanent mental changes long after the person is abstinent. PCP psychosis can persist for months after chronic abusers stop using. Longterm alcohol dependence can result in permanent memory deficits. These residuals problems
can be used as the basis for a legal defense.
Another legal theory that allows for substance abuse is the idea of involuntary intoxication---what I think of as the "mickey" defense---meaning that you took something without knowing it. Drinking spiked punch or accidentally taking the wrong pill might be an involuntary intoxication. Having an unusual or rare reaction to a medication---like an SSRI---could be a type of involuntary intoxication defense. Something like this would be more common with other drugs, however, with the classic one being steroids. About 15% of people prescribed prednisone have a dose-dependent affective side effect. When the first case studies were published about the psychiatric effects of anabolic steroids there was a flurry of criminal defenses based on this. Later research showed that the people who were more prone to 'roid rage' where people who also had antisocial personality disorder.
The final issue you'll hear about is the idea of paradoxical intoxication, in which a person has an extreme reaction to a small quantity of a substance. Roy mentioned the cases of homicide or robbery after only two doses of an SSRI; this would be an example of proposed paradoxical intoxication defense. (Actually, the best example of paradoxical intoxication I've seen is the movie
Final Analysis. It's also a good illustration of the kind of criminal defendants who propose defenses like this.)
So that's my input. Pass the Paxil and stand back!
Dinah:
What never fails to amaze me is not that people have side effects or adverse reactions to medications, but the great variety of responses people can have to the same medication. If 70% of people will have a given response to a medication (hmm, let's say dimunition or resolution of depressive symptoms if we want to look at the cheery side of things, or sexual dysfunction if we want to look at the gloomier), well what about the other 30% of folks? Why is it that some patients have a great clinical response and there is no down side? Some people seem to be more medication-sensitive in that they are more prone to side effects or need lower doses of medicines, but there isn't necessarily carry-through from one class of drugs to another. So, we all know that Lithium may cause weight gain, but I've seen patients on high doses of lithium for years that haven't gained any weight, and we all know that zyprexa may cause weight gain (note that I say "may" because it's just not a given), so why will the same patient might tolerate one of these with no problem, and start piling on the pounds when you switch to the other?
Roy's reference gives several explanations as to why SSRI's might induce violent behavior: switch to mania (perhaps with psychosis), akathesia, activation, emotional numbing. Clinically, the question of SSRI-induced suicidal/homicidal behavior has always been a tough one: these medications aren't prescribed to people who are trooping along Just Fine. Suicidality is a very common symptom of Depression and SSRI's are prescribed for depression; we're left wondering if the SSRI caused the suicidality, began working and lifted the patient to the point of being able to act on the thoughts, shifted the patient into a bipolar mixed state, or simply was ineffective in treating the depression and was incidental to the final act.
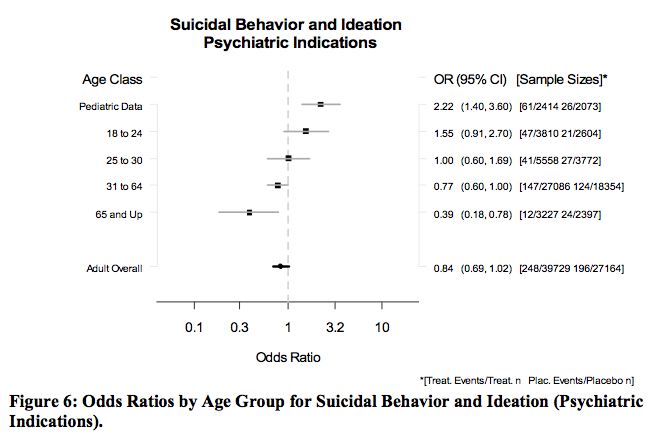
Given the vast range of odd side effects/adverse reactions that people get from medications, the studies linking
suicidal ideas in children to SSRI's and the extreme nature of the cases discussed in the PlosJournal article, it's probably reasonable to say that a very small percentage of patients given SSRI's may become violent. Still a bit of a stretch for me, because there are also people who have no history of violence who unpredictably kill someone, and it becomes hard to look at the correlation to a medication when tens of millions of Americans take that medication (kind of like I eat Twinkies and I didn't kill anyone) and only a few of them unpredictably become violent.
And what does this mean clinically? I think I'm left to say something fairly flat, like: Not Much, So Far. I don't work with children, where I believe the implications are broader-- the black box warning on SSRI's regarding suicidality may be giving pediatricians a moment's pause before prescribing them, and the latest recommendations suggest that kids be seen fairly often for the first month of treatment: probably not a bad idea, though perhaps cumbersome given the shortage of child psychiatrists.
To date, I have not seen a previously nonviolent adult become violent on an SSRI. People still enter treatment asking for these medications, and many people find they effect life-altering changes for the better. Some people have no response at all. Some people feel much calmer, less irritable, and better able to cope with what life throws them. Some simply cease to be depressed and identify that the medication makes them feel like their old, pre-depressed self. Often, people have sexual side effects and are left to make a decision. If someone were to report violent ideas on the medication, as with any distressing side effect, I would discontinue it. For an out-patient practice, the decision to take or not to take medications is ultimately the patient's; I can discuss the possible risks and the possible benefits, I can make a recommendation based on studies I've read and patient responses I've witnessed, I can strongly encourage someone to take medications, and ultimately I suppose I could refuse to treat someone who I felt I couldn't help at all without medication, but the final decision is generally an issue of team work, and often the patient comes in predisposed: "I'm never taking meds" or "Prozac made my best friend better and I want some of that stuff."
The vignettes in this story are striking. To date, I've not felt a need to warn patients that they might become violent: these cases are the exception, not the rule, not anywhere close. If I hear enough of them, I'll start warning people, until then, I'll leave it to the ever-present media, and I'll keep a close eye on my patients.