I'm coming up for air and a quick blog post. For the last couple weeks I've been codestorming, lost in a flurry of flow-control statements, if-then and for loops, switch blocks, dropped semicolons and variant datatypes (cursed be he who invented the variant datatype for to such belongs the world of sloppy programming). After 18 months waiting for the bureacracy to give me a regional information system I can use I finally gave up and built one myself. It took two weeks. Meanwhile no one in my department has ever been able to use the system we're supposed to be using. It's enough to make a taxpayer cry. Anyway, my personal system is pretty much done except for minor cosmetic tweaking.
But that's not what I was going to blog about.
Today I wanted to talk about what happens when you run into your patients outside of professional hours. In my case, it can be interesting.
I went to the post office to mail off my taxes and I noticed someone standing toward the front of the line who looked awfully familiar. Thanks to my recent accident I've been meeting a lot of car salesmen lately, so I was thinking it was maybe some business person or a public defender type. Then it hit me---a former inmate. He either didn't recognize me or was reluctant to acknowledge me, which was understandable. In a public place you just don't strike up conversations about your former incarceration, much less about your mental health care even if you haven't been locked up.
Generally meetings with former inmates are fine if I run into them on the street. Usually they recognize me first since I get thrown once you take someone out of a prison uniform and put them in street clothes. I usually hear about how things are going "on the outside", whether or not they've been able to get mental health care, how long they've stayed clean and how much time they have left on parole. They seem happy to see me and I like hearing about how they're doing. Even when they're not doing so well they seem happy to see me. The most awkward meeting was coming across a former patient a the time of arrest, handcuffed and prone on the street in front of my parked car. "Hey doc! I'm going to need your help!" he said. I reassured him I'd be there when he got to the institution and reminded him how to get in touch. He said he would.
Overall I'm grateful I only work in men's facilities. It kind of spares me from thinking about running into former patients in the locker room at the gym.
Tuesday, February 27, 2007
Sunday, February 25, 2007
My Three Shrinks Podcast 12: Bilingual

We had two other topics recorded from a prior session, one on the side effects of psychotherapy and the other on the street value of psych drugs in Las Vegas, but GarageBand somehow lost them (I really don't think it was me.) If I find them later I'll put them out in a podcast.
As a result, this one's shorter... about 18 minutes.
February 25, 2007:
Topics include:
- Evolutionary Psychopathology. LA Times article, The Mind as it Evolves, by Julia M. Klein, about a developing area that theorizes that the illness of depression developed as an evolutionary strategy, which helped signal and stabilize social ranking. Very interesting reading. See also the journal article, The evolutionary significance of depressive symptoms, by Matthew Keller and Randolph Nesse from VCU.
- Mental Health Parity Act of 2007. Well, we have been trying to get this passed for years (see NAMI's review), despite popular bipartisan support. It passed the Senate, and will hopefully pass the House for the president's signature. We also talk about Maryland's 1993 landmark parity legislation.
- Psych Blog: Psychiatry for All, by Saminkie. A psychiatry resident in Baghdad who writes about learning psychiatry while having to deal with bullets, explosions, no electricity and other war-related problems. (Sent to us by DrivingMissMolly.)
- The Psychiatrist Blog, by Michelle Tempest. A UK psychiatrist, and author of The Future of the NHS, blogs about psychiatry, health and politics.
Last week's musical snippet was from Monty Python -- Spam; and Finland, Finland, Finland.
Find show notes with links at: http://mythreeshrinks.com. This podcast is available on iTunes (feel free to post a review) or as an RSS feed. You can also listen to or download the .mp3 or the MPEG-4 file from mythreeshrinks.com. Thank you for listening. |
I'm Not Old

I was eating lunch with a friend the other day. She was talking about her sick friend, her husband's upcoming big birthday, her mid-life crisis of sorts.
"I'm not looking forward to this next phase of life," she said.
"Huh?"
"Getting older. What's to come."
"Getting older. What's to come."
Age, I've decided after years of watching people, is a matter mostly of luck and partly of mindset. Mostly of luck. I've seen people who are old by 40. I've seen people in their 70's, and sometimes even 80's, who are still full of life. I recently treated a man in his early 90's who still had stuff going on.
"I'm not getting old," I said. I feel fine, why would I spend my time thinking about impending disability.
My friend is a runner, she's tall, slim, beautiful, and has two sons in elementary school. She looked at me shocked.
"You're my age. You're in denial."
Perhaps I am. My children, especially the younger one, tell me I'm old at every turn. Actually, I'm a bit younger than most of their friends' parents. I tell them so, it bounces off and lands with a thud.
Back in the day, I think. I can remember, and I'll leave you with a list:
Going to the library to do research out of books.
Finding those books after looking them up in the big card catalogue which took up half the room.
Finding journal references in The Readers' Guide To Periodic Literature (or something like that) and reading the reels on microfilm.
Answering the phone, attached to the wall.
Not knowing who was calling until you actually answered.
Dialing. Really, dialing.
Staying home to wait for a call.
Using pay phones, routinely.
I was in med school the first time I saw a cell phone. It looked like a vacuum cleaner. Well, not really.
Television in black and white, though the neighbors had color.
Getting up to change the channel.
TV Kids who said "Golly Gee" and no one cursed.
Saying to my big brother: "I turned it on, you turn it off," when no one wanted to get up.
Saying to my big brother: "You turned it on, you turn it off," when no one wanted to get up.
Television shows that had to be watched when they aired, not on video tapes or TiVo.
Movies on big screens only, as double features.
Radio: shaped like an orange ball that played AM only. Taking it to the beach.
Records that came as 45's and 33's and got scratches.
Oddly enough, all the recording artists were the same then as now.
Riding in cars without buckling the seat belts. (I don't remember ever being in a car that actually didn't have seat belts).
Cars where you stuck the key into the lock to open the door.
Cars with roll down windows.
Typewriters. I remember typewriters. I even remember manual Smith Coronas. I remember carbon paper and erasable paper. (Oh my God, I AM old.)
Keypunch and all those keypunch cards. I remember COBAL.
Huge computers that filled cold rooms. Something called DEC-10.
Volkswriter, and then WordPerfect.
Elavil and haldol and there was no Prozac, no atypical anti-psychotics.
Patients stayed in psychiatric units for weeks to months, and even years.
I remember psychiatric units with Adirondack chairs on the lawns and patients went home on overnight passes.
Psychiatric residents who routinely had personal analyses (this may have been a New York thing).
I remember classrooms filled with wild little boys who didn't take stimulants.
I remember a time when I'd never met a child with autism. Learning about autism in college, a very rare condition.
I remember Tab and the world before Diet Coke. Cheerios were unflavored and the only bread was white bread. Scooter pies, Pop tarts and plastic Twinkies tasted good, but Cap'n Crunch ruled. Ronald McDonald toured and lines ran around the block.
So maybe I am old. Someone, please hand me my cane.
Saturday, February 24, 2007
Home Work

This is for our obstetrician blogger friend who wanted some help with her homework: preparing a lecture for OB/GYN residents on psychiatric issues in pregnant women.
-----
I'm going to ramble (I'm good at that), no references, no specifics.
What do we do about psychiatric disorders in pregnant women? This is a tough question, mainly because we know so very little, it's not unlike the issues that get put forth regarding the efficacy and safety of treatments in children: both are populations that don't get experimented on. To figure out the teratogenic effects of medications (one option in treatment) on the unborn fetus, studies are done on pregnant laboratory animals, which often tell us little about the effects on unborn people. We simply can't design studies that purposefully expose pregnant women to medications and ask Hey What Happens to those kids. What we know is incidental: someone taking the medication gets pregnant, it's reported, outcomes are followed up on. Little is known about exposure at varioius times during fetal development, and outcome is generally limited to structural birth defects and behavior in the immediate post-natal period. So there's nothing that says that a 6 week old fetus exposed to psychotropic drug X is more likely to have reading delays at age 7 or coordination problems or is less likely to fill-in-the-blank. And just to make the story more complicated, we also don't know what effects untreated maternal mental illness have on the fetus, so even if there is some risk from medications, it's looking like very sick mothers aren't good for babies, and maybe the risk of treatment with medication may be better than the risk of not medicating, but this remains speculation as these issues are only just beginning to get the attention they deserve.
------
Any way you dice it, I think an obstetrician needs to refer a mentally ill pregnant patient.
----------------
From my shrinky perspective, I believe the fetus should be exposed to a minimum number of Unnecessary medications, I think they are all Potential toxins. I tell pregnant patients that the threshold for medication is raised: I ask them to tolerate some distress for the sake of the baby, we do this anyway. We ask pregnant women to give up all the essentials: cigarettes, alcohol, otc medications, Diet Coke, street drugs, Diet Coke, coffee, hair chemicals. Perhaps we ask pregnant patients to tolerate symptoms of mild depression or anxiety or sleeplessness that we might otherwise offer medication for. The threshold for psychotherapy should also be lowered: talking is unlikely to harm the fetus, frequent sessions provide an outlet for the patient and a means to increase coping mechanisms, and systems are set in place for the therapist to do on-going evaluation and monitoring. Other support systems need to be shored up: family members often must be called upon and all available resources may be needed. A therapist may need to work with the patient on the importance of taking care of herself and accepting help from others: often a difficult thing for moms to do.
------
Sometimes, issues related to coping and expected discomfort can be confused with symptoms of mental illness. A woman is sad, tired, nauseated (for Fat Doctor), not eating well, crying. Does she tell her obstetrician that she and her husband are fighting non-stop, that her co-workers are angry about her pregnancy, that the other 5 kids are overwhelming, or does she simply say "I'm depressed," a self-made diagnosis that may or may not be right and may or may not need medications?
---------
Sometimes, there is no escaping medication: a pregnant woman is so symptomatic that medication must be given. We don't leave patients psychotic (hallucinating or delusional) or manic, or terribly depressed; in these instances we offer medication and do our best to work with what we hope will be safe and we avoid those meds we know are not. I'll leave the lists to you, but the patient gets the best care when the psychiatrist and the obstetrician work together.
So why do I think you should refer? I'll give it to you as bullet points:
- OBs don't spend the time with patients needed to make an accurate psychiatric diagnosis and this is essential.
- OBs don't generally have a good enough handle on diagnosis and treatment of psychiatric disorders to be doing it. (And I don't catch babies).
- If the baby has a bad outcome for any reason, a defense attorney will have no problem targeting an OB who treated a psychiatric illness in an expecting mother.
- If the mother does something horrible because of untreated or wrongly-treated mental illness, this can be catastrophic.
- OB's typically stop seeing the patient 6 weeks after delivery and the patient will need on-going psychiatric care.
----
When do you refer?
- If the patient appears to be having psychiatric symptoms that are endangering herself or the baby: a sad mom who isn't gaining the necessary weight due to poor appetite, one example.
- If the patient mentions suicide or harming the baby or any pre-existing children.
- If the patient says she thinks she has a psychiatric disorder or names an illness.
- If you even wonder if you should refer. Phrase it as an evaluation: I'd like you to see a psychiatrist one time just to get a handle on whether there is even a problem.
To our OB friend, I hope this helps.
Friday, February 23, 2007
Nine Months And Counting....And Counting...

I started this post as an email to Midwife With A Knife to help her with her talk about perinatal psychiatric issues. It got long enough that I decided to turn it into a blog post instead. I see Dinah is also working on her part of MWAK's homework and it's a good one. Here goes.
Last November I went to an excellent CME lecture on perinatal OCD. I thought this would be a nice change from the usual maternity-associated illnesses like post-partum depression and psychosis.
First of all, obessive-compulsive disorder is an anxiety disorder characterized by obsessions or compulsions that are time consuming or interfere with social or occupational functioning.
Obessions are anxiety-producing thoughts, impulses or images that are excessive and beyond the range of normal worry about real-life problems. Sufferers usually recognize that they are irrational, and often try to ignore or suppress them. The most common types of obsessions are contamination obsessions followed by obsessions about aggression or the need for exactness.
Compulsions are urges to perform repetitive behaviors or mental acts. They usually happen in response to obsessions and are aimed at reducing distress or preventing some unpleasant event. The most common types of compulsions are checking rituals followed by cleaning or washing. There can also be mental compulsions (repeating words or numbers, counting or reciting prayers.)
The prevalence of OCD is about 1 in 50 people (2.3% of adults). The gender ratio is 1:1 male/female. The prevalence of perinatal OCD is 0.2 to 3.7%. Eighteen percent of new cases occur during the postpartum and 6% during pregnancy. Most women with pre-existing OCD have no change in symptoms with pregnancy, but one-third may have worsening or a change in symptom presentation.
The types of obsessions in perinatal OCD are different than in non-postpartum OCD. Postpartum obsessions are more likely to involve contamination fears or fears of violence (eg. intrusive thoughts to poke the baby's "soft spot", putting the baby in the microwave) than non-postpartum OCD. Patterns of compulsions are also different---postpartum OCD is more likely to involve checking, washing and cleaning rituals. Some OCD patients have been known to call their daycare multiple times a day to neutralize their obsessions.
About half of women with post-partum depression have co-existing OCD, but the OCD is less likely to be diagnosed because of patient concealment and embarrassment. And yes, fathers can get it too.
Treatment usually involves cognitive-behavioral therapy sometimes combined with medication. For the Ob-Gyn crowd, this would be the time to refer. Dinah is writing a good post about meds in the peripartum, so I'll leave that to her.
Hope this helps.
Why Docs Don't Like Xanax (some of us)
[BTW, you might also be interested in checking out our related podcast, #19: Xanax Blues.]

This is in response to JW's question below about the "rules" docs use about prescribing Xanax/alprazolam. Not all docs feel this way, but here's how I think about it. Of course, I am not suggesting that, if you are taking this anti-anxiety drug, you should stop it. I'M NOT. Talk to your doctor if you have concerns.
The half-life for Xanax is short... on the order of 6-20 hours. Halcion is the only similar sedative that has a shorter half-life (and that one has even more problems). Thus, it doesn't stick around long. It is also quite lipophilic, meaning that it quickly gets into the brain. So, it has a quick on, quick off way of working. Sounds great, right?
The quicker a drug works, especially one which makes you feel good in some way, the more addicting it is, as the cause (taking it) and effect (feeling it) are close in time, making it very reinforcing. This is fine if you just take it on those rare anxious moments where you need something to get through it. However, since it works so quickly, many folks start taking it more and more often, until it gets to the point that they are taking it daily. Then they start taking it as soon as they feel it wear off. Before you know it, you are taking it 3-4 times per day. Now, that's not the big problem.
The big problem is all because of your brain's laziness. See, your brain makes it's own natural Xanax-like substance, called GABA. GABA works by inhibiting the brain's natural tendency to speed up. It's like a brake pedal, where the accelerator is stuck in the pedal-to-the-metal mode. GABA keeps your brain from over-working. Xanax (and other sedatives, and alcohol) works by acting like GABA in the brain (sort of). If you start taking it daily, your brain starts thinking "I guess I don't need to make so much GABA because this Xanax stuff is here, so I'll only make 20% of what I usually make." It takes a week or more for your brain to stop making the GABA (which is why just a few days on Xanax won't lead to much trouble), and a week or more for it to start making it again when you stop taking the Xanax.
Here's where the trouble begins. If Xanax wears off in just a few hours, but it takes a week for your brain's natural Xanax to kick back in, what happens in the interim? Withdrawal. What does that feel like? It feels like a panic attack, but worse. High blood pressure, rapid heart beat, tremors, confusion, delirium, hallucinations, seizures. What do folks do when they feel a panic attack coming on? Take another Xanax.
As a hospital-based physician, I see lots of folks, often older, who wind up with severe withdrawal problems from Xanax. It's usually because they run out of the drug, decide to cut back or stop taking it, or something else happens (eg, stroke, get sick) and they forget to take it. Or they don't tell their surgeon they are on it, and 2 days after their hip surgery I get called because they are hallucinating.
Some prescribers think it is a good antidepressant (it's not). Or that, because of the short half-life, it's not as addictive (it is).
So, here are my rules of thumb about Xanax:
The half-life for Xanax is short... on the order of 6-20 hours. Halcion is the only similar sedative that has a shorter half-life (and that one has even more problems). Thus, it doesn't stick around long. It is also quite lipophilic, meaning that it quickly gets into the brain. So, it has a quick on, quick off way of working. Sounds great, right?
The quicker a drug works, especially one which makes you feel good in some way, the more addicting it is, as the cause (taking it) and effect (feeling it) are close in time, making it very reinforcing. This is fine if you just take it on those rare anxious moments where you need something to get through it. However, since it works so quickly, many folks start taking it more and more often, until it gets to the point that they are taking it daily. Then they start taking it as soon as they feel it wear off. Before you know it, you are taking it 3-4 times per day. Now, that's not the big problem.
The big problem is all because of your brain's laziness. See, your brain makes it's own natural Xanax-like substance, called GABA. GABA works by inhibiting the brain's natural tendency to speed up. It's like a brake pedal, where the accelerator is stuck in the pedal-to-the-metal mode. GABA keeps your brain from over-working. Xanax (and other sedatives, and alcohol) works by acting like GABA in the brain (sort of). If you start taking it daily, your brain starts thinking "I guess I don't need to make so much GABA because this Xanax stuff is here, so I'll only make 20% of what I usually make." It takes a week or more for your brain to stop making the GABA (which is why just a few days on Xanax won't lead to much trouble), and a week or more for it to start making it again when you stop taking the Xanax.
Here's where the trouble begins. If Xanax wears off in just a few hours, but it takes a week for your brain's natural Xanax to kick back in, what happens in the interim? Withdrawal. What does that feel like? It feels like a panic attack, but worse. High blood pressure, rapid heart beat, tremors, confusion, delirium, hallucinations, seizures. What do folks do when they feel a panic attack coming on? Take another Xanax.
As a hospital-based physician, I see lots of folks, often older, who wind up with severe withdrawal problems from Xanax. It's usually because they run out of the drug, decide to cut back or stop taking it, or something else happens (eg, stroke, get sick) and they forget to take it. Or they don't tell their surgeon they are on it, and 2 days after their hip surgery I get called because they are hallucinating.
Some prescribers think it is a good antidepressant (it's not). Or that, because of the short half-life, it's not as addictive (it is).
So, here are my rules of thumb about Xanax:
- Avoid it.
- Keep the doses small.
- Do not use in older folks or forgetful folks (more likely to forget it, thus more likely to have problems).
- Do not use in anyone with a history of alcoholism or addiction (yes, that means you have to ask).
- Tell folks to avoid from daily use.
- If they are on it, warn them that stopping it suddenly, even for a day or two, can result in confusion, hallucinations, seizures, and even death.
Tuesday, February 20, 2007
The Top 10 Things I Don't Like About Being A Shrink
I'm doing this alone-- my co-bloggers are welcome to post their own-- because finding and then nagging Roy is a full-time job. Still waiting for the carpenter to come put things back after we dragged him out to say why he loves his job.
I love my job, as mentioned below in Who Wants To Be A Psychiatrist. But every thing, every job, every relationship, every new or old endeavor, has it's down side, and so this is to present a more balanced side of what I generally think of as my blessed life.
I love my job, as mentioned below in Who Wants To Be A Psychiatrist. But every thing, every job, every relationship, every new or old endeavor, has it's down side, and so this is to present a more balanced side of what I generally think of as my blessed life.

The Top Ten Things I don't like about being a Shrink:
10. Filling out HCFA forms for Medicare over and over and never knowing why they're rejected.
9. Chronic benzodiazepines. The ones that fell down the sink. Why don't zoloft prescriptions ever run out early?
8. The heating unit in my office is awful. It's loud and the room is always too hot or too cold -- this has persisted after it was replaced with a new and improved unit.
7. Arguing with ClinkShrink about who deserves care and what an illness is.
6. No place to lock my belongings in the clinic where I work so I carry my purse everywhere.
5. Wondering if I'll live through eight psychotherapy sessions in a row when I've forgotten to schedule myself a lunch. Or worse, remembering to schedule a lunch, then only having one patient after that, and the patient right before lunch cancels, leaving me two hours of dead space before the last session.
4. Nonsensical paperwork in the clinic.
3. The work of seeing patients who don't talk spontaneously and look to me to guide the entire session, then answer any questions I can think of in single sentences. These can be long sessions.
2. The chaos of patients who simply don't show up or who repeatedly cancel at the last minute. Especially if the reason is that it's the only time they could get an appointment with their hairdresser.
And the Number One thing I don't like about being a psychiatrist.....
1. Talking about unpaid bills, which I have on ocassion let go much longer than I should.
Sunday, February 18, 2007
My Three Shrinks Podcast 11: Lovely Spam
We almost didn't make a podcast this week, as both Dinah and Clink were under the weather; but I brought my hazard suit and gel scrub and we managed to complete it. It did go a bit long, about 50 minutes.
February 18, 2007:
Topics include:
- FDA Antidepressants Hearing, Revisited. We had previously blogged about suicide and antidepressants, followed by Roy's first-hand account of the December 2006 FDA hearing which Roy attended, where the committee voted to expand the black box warnings on antidepressants to indicate the risks of untreated depression and to mention the protective effects that antidepressants appear to have on older folks. The FDA has now released two transcripts of the hearing (Transcript 1 and Transcript 2), as well as the slide presentations from some of the speakers. These are excellent resources if you want to find out more on the subject. The recommended changes (see summary) to the black box include text to highlight the following:
- increased risk of antidepressant-associated suicidal thoughts and behaviors up to around age 25
- protective effect of antidepressants against suicidal thoughts and behaviors for older folks, particularly seniors
- balancing language which points out the increased risks associated with NOT treating depression (eg, suicide rates have increased for children since the 2004 decision to add black box warnings for antidepressants)
- Finland, Finland, Finland. The Finnish study that Dinah mentioned is discussed here. The Monty Python audio was found here.
- The Zyprexa Documents. The FuriousSeasons blog details the concerns that Lilly is holding out on important information about its antipsychotic drug.
- NYT: Bipolar toddler dead from medications. Raises questions about diagnosing severe mental illness in very young children.
- Lovely Spam. on YouTube.
- Q&A at mythreeshrinksATgmailDOTcom. Schizoid personality disorder: Is it real and does it predispose to schizophrenia? By Seamonkey. Diagnostic criteria. Pubmed review.
- Amygdala size and eye contact in Autism.
- Asperger's syndrome.
Next week: Side effects of psychotherapy; evolutionary psychopathology; what happens in Vegas.
Last week's musical snippet was from the 2000 release, Strangelove Addiction, from the self-titled album by Supreme Beings of Leisure.
Find show notes with links at:
http://psychiatrist-blog.blogspot.com/2007/02/my-three-shrinks-podcast-11-lovely-spam.html
This podcast is available on iTunes (feel free to post a review). You can also listen to or download the .mp3 or the MPEG-4 file from mythreeshrinks.com. Thank you for listening.
Saturday, February 17, 2007
Switched-on Blogger (2.0)
Well, it seems we made the switch, but darned if I could tell the difference. Where's the cool drop-down selectors for the archives and for the blogroll?
I'll check out the Template area, maybe there's something there. This whole widget business looks interesting, also. If any of our readers have some good tips about using the new Blogger, especially the widget feature, please comment.
Oh, Dinah is under the weather so we might not make our podcast tomorrow.Thursday, February 15, 2007
Who Wants to be a Psychiatrist?

[begun by dinah]
There are lots of wonderful things about being a psychiatrist.
Is this a good way to start a post? Seriously, there are. The med school stereotype includes real downers, and not that many docs go into psychiatry: All psychiatrists are crazy (I would say Most psychiatrists are perhaps a little odd, present company excepted, but what's the thrill of being "normal"?). Psychiatric patients don't get better. This is just wrong: they do get better and many are effusive with their appreciation. Psychiatrists don't get paid well. Umm, compared to the neurosurgeon who gets thousands for an operation, that's true. Okay, shrinks are at the bottom of the doctor pay-pole, but money isn't everything.
So this is what's great about psychiatry: the field is huge. One can become a psychoanalyst, never touch a patient, never prescribe a medication (still? not sure, I'm not a psychoanlyst and only know a handful), see patients 4 or 5 times a week (rich ones) to get to the bottom of their defended conflicts: this is all Art and No Science. One can see patients in a multitude of settings ranging from prison to public clinics to private offices, inpatient, outpatient, partially hospitalized, college health clinics, emergency rooms, psych hospitals, general hospitals, or everyone's favorite: hospitals for the criminally insane-- okay, okay, ClinkShrink says I have to call it a secure forensic facility. One can become an an administrator and never deal with a live patient. Or an academic researcher and write grants, run clinical trials on patients, or study neurotransmitters and receptors and also have little to do with whole people--this is all Science and a little Art. There's room as a psychiatrist for a second life: parent, novelist, fine artist, even blogger. I suppose that's true of other medical specialties as well, but psychiatry tends to attract (some) folks who are interested in the introspective, the artistic side of life and its creative outlets. Am I right? No clue.
I write a lot about doing psychotherapy. It's not all I do, I write a fair number of scripts and I've always identified myself as a community psychiatrist--a shrink who works in publically-funded clinics with chronically mentally ill patients. I was even an administrator for a while there-- But I like to write about psychotherapy, I think because it's illusive, it's hard to pinpoint why it's helpful to talk to someone, how it effects cure or change or even what value we place on comfort in the absence of cure or change.
And why do I like doing psychotherapy? In a word, intimacy. Nowhere do people touch so close, let you in with such trust, then change and get better not because of a drug, or just because of a drug, but because of what you do with your being: listen, reflect, and sometimes just care.
[ClinkShrink says:]
I was destined to be a forensic psychiatrist. I didn't know it at the time, but growing up on a steady diet of Agatha Christie, Ellery Queen and Arthur Conan Doyle (not to mention Ed Gein jokes) pretty much determined my professional future.
When I was in medical school I never planned to be a shrink. I was considering almost everything else---emergency medicine or oncology being the foremost---until I took my psych rotation. It was the high point of my medical school experience. I had some pretty amazing and unusual cases (even compared to what I've seen since then), including one famous case involving a patient who is still discussed in forensic training programs. Our civil commitment hearings were held in an actual courtroom so as a medical student I also got to see my first expert testimony in front of a real judge. One of my progress notes was even quoted at the hearing. Pretty darn cool.
Meanwhile I saw residents in other specialties dragging their butts around the hospital exhausted and demoralized. While they intellectually liked their specialties they just didn't seem happy. Psych residents, on the other hand, loved what they were doing and smiled a lot. They also tended to have delightfully twisted senses of humor. I fit in there.
I've never regretted my decision. I still like my patients and my colleagues. I still like the predictable chaos of institutional work and the knowledge that I'm doing the right thing. It's fun to see people gradually get better and to know you had something to do with it. When I hear an interesting delusion I wonder why anyone would want to do anything else. And I particularly liked it today when my patient told me, "Thanks, doc. You're a blessing. You really are."
Pretty darn cool.
[finished by Roy]
Fine, I'm being forced to talk about why I like being a psychiatrist, by threat of emasculation. I'm not going to talk about why I became a psychiatrist, but why I love it. Keep in mind I'm a Consultation-Liaison psychiatrist (also called psychosomatic medicine), which is essentially psychiatry in the general hospital. I see all sorts of people with all sorts of problems, from the mundane to the fascinomas. You get to help solve problems by thinking of things in ways others haven't. It's a bit of Sherlock Holmes plus Marcus Welby, with some Dr Huxstable and a bit of House thrown in.
I can do any kind of psychiatry I choose (inpatient, outpatient, administrative, research), in any type of practice (solo private practice, group practice, clinic, hospital-based, large single specialty practice), part-time or full-time, and pretty much always be able to get a job that pays well while being independent enough to be able to vote with my feet if I disagree with how an employer treats patients. I have, in fact, done all of the above at various times (as Dinah can attest), sometimes many of them at once.
At one point I thought of being a psychologist, but found it too theoretical, and it didn't answer all my questions about how the brain works, how the body works, etc. The best part is being a physician and having the confidence of knowing the difference between, say, a seizure and a pseudoseizure, because I learned about both these things, learned how to examine for these things, and know the importance of getting it right or wrong.
At another point I thought of becoming a neuroscientist, but found that I missed the people contact. I really like working with folks whose brain is on the fritz, and helping them get their picture back so they can enjoy life more. That is satisfying.
(I hope Dinah's happy now :-)
-------------------------------------------------------
And now that you've heard why we all love our jobs
And now that you want to be a shrink, too,
I thought I'd post
This poem for you.
{kind=link}
Wednesday, February 14, 2007
A Special Kind of Relationship

We've had a whole series of posts on psychotherapy, what gets said, who should have it, who should do it, and does it matter what gets said. I'll put some links below for anyone who's missed out on the sometimes heated discussion.
We've talked about why it would help for someone to come to treatment and talk about their day to day activities, and I've mentioned a confabulated patient who talks about the price of beef (comparative, of course, checking out the sales at various grocers) and we've wondered how that might help.
Sometimes it's about what gets said: the act of saying something effects the cure. This can be particularly true if the problem is directly related to an event-- secret, traumatic, tragic, or just plain troubling.
Sometimes it's about what gets said: a patient listens to himself and figures out his own solutions. The therapist is a sounding board and the patient does all the work.
Sometimes it's about what gets said: a therapist can point out patterns in a patient's feelings, interactions and reactions, and it helps when such patterns, unseen by the patient, are elucidated. Maybe the patient can change these patterns if he's aware of them, or maybe there's something about us that just likes being understood with a sprinkling of those "ah ha" moments. People like it when a therapist is able to say: "You're the type of person who...." and the therapist is right. Patients especially like it who the thing they're hearing is something good, such as "You're the type of person who cares deeply about others." It's feels a little bit magical when a therapist does this in the first session, especially if they hone right in and put into words something that hasn't been put into quite those words before.
Sometimes, it just doesn't matter what gets said.
It's about the relationship.
I've been wanting to write about this for a while. I haven't because, well, I haven't known what to say. There are all sorts of things that have been said about why the therapeutic relationship helps, mostly unproveable, some just feel wrong, or it feels like the therapist is trying to force the pieces into the puzzle. Unconditional Positive Regard? I'm not sure that ever really happens and it wouldn't feel genuine. In fact, a mandate for unconditional positive regard entails dictating the therapist's feelings in a way that might call for dishonesty. The idea that the therapist is consistently present and accepting of the patient's difficult feelings is helpful, though I'll point out that such consistency comes at a price, a literal by-the-hour dollar figure, and really, there are no guarantees-- therapists move, quit, get sick, and even die. We just like to think we offer consistency and acceptance (and that we don't die).
What therapy (or at least good therapy) does offer is a safe place to talk about difficult stuff. It's essential that the patient feel that the therapist either understands him or is trying very hard to understand him, and I believe that it has to be an honest relationship-- a safe place to hear things one might not otherwise be willing or able to hear. It's a narcissistic endeavor, it's all about the patient, and that's how it should be. I use the word narcissistic loosely here --I could probably find a better, more accurate, and less loaded word, but I like this one. In friendship relationships there's a give and take-- I tell you my story and if you're a guy, You tell me how to fix my problem. If you're a girl, you tell me about the time something happened to you that was just like what just happened to me. Either I get an answer or I get some much-needed empathy, but either way, I hear about You.
I could talk about transference helps a patient to understand and work through difficulties in past relationships as they play themselves out in the here and now. Really, I can talk about it, it even sounds good, I just haven't found that it plays out in therapy the way it sounds like it should, at least not as a neat package where I can articulate each step.
I'm left to ramble.
Sometimes it's about the relationship. I don't always know why.
Happy Valentine's Day from the shrinks at Shrink Rap!

Links to past posts about psychotherapy:
Talk Therapy
What Makes It Therapy?
What People Talk About In Therapy
ClinkShrink's Couch Time
Transference To The Blog
Tuesday, February 13, 2007
Happy Valentine's Day! Think Hearty

OK, people want Valentine's Day posts so hear goes.
While everybody was out buying candy and flowers and cards I celebrated Valentine's Day in a slightly different way---I got recertified in CPR.
Yes I know, how romantic!
But think about it---what better way to show someone you care than to be prepared to save their life? According to what our CPR instructor said, most CPR is done on people we know---family members, friends or co-workers.
And yes, re-training is necessary. I was pretty surprised by what they're teaching now. It's changed quite a bit just in the past year. The Red Cross and the American Heart Association have simplified the resuscitation guidelines quite a bit and it's a lot easier to learn now. All those complicated ratios about compressions-to-rescue breaths for the adult, child and infant have been boiled down to one simple rule: 30 compressions to 2 breaths for all. And no more finger sweeping of throats---if someone is an unconscious choking victim you go right to CPR. Of course, much of the emphasis now is on automatic external defibrillator training. If you've never had a chance to try this you really should---it's kind of a hoot. The little machine talks in its little machine voice and tells you what to do step by step. (My little geeky imagination can't help fantasizing about things you could reprogram that machine to say, but I digress.)
And while we're on the topic of hearts, in honor of WoodburyMomAndPop I'd like to remind everyone that February is Women's Heart Health month. Go the the American Heart Association web site here and check out your numbers---the first step to prevention is to know your risk factors.
And Woodbury, you make a great TV talking head. I may eventually get used to seeing you in makeup.
Quiet Time
 [posted by dinah, who finally got into the dashboard]
[posted by dinah, who finally got into the dashboard]There are many people in my life-- even among those who love me--who would like just a little peace. "You talk too much." I've heard that at times. Oh, lots of times. An occupational hazard, I like to rationalize, of having to sit quietly and listen so much.
So now, even blogger, from 3 different computers, wants me silent. Surprisingly, I'm doing okay with it, waiting patiently for Clink & Roy to update us, biding my time. I've only had a few seizures, petite mal at that, and I'm almost caught up on LOST : up to beginning of the third season at any rate.
It's not that I have much to say, it's just that, well, that's never stopped me before.
Clink, Roy, any time it's safe to update to the new, improved, and postable Blogger, just say the word.....
Sunday, February 11, 2007
My Three Shrinks Podcast 10: Be Mine
Valentine's Day is soon upon us. Hearts, flowers, and chocolate abound. This got us three shrinks wondering about why chocolate holds such a high position in this whole love-related endeavor.
We talk about the psychopharmacology of chocolate, while we simultaneously try a taste of own pharmacocoatherapy.
Oh, and this is our TENTH PODCAST! (woo)
February 11, 2007:
Topics include:
- AJP: False positive drug tests on Effexor XR (venlafaxine) (positive for PCP, or phencyclidine).
- Chocolate and Mood [PubMed]: a look at chemicals in chocolate which affect mood, such as theobromine, caffeine, phenylethylamine (PEA), and anandamide.
- First study mentioned by Clink, on chemicals in chocolate.
- Second study, about mood modulation by food.
- Third study, about chocolate and atypical depression.
- Green M&Ms. Also, design your own M&Ms, even what is printed on them.
- Dogs: Don't eat the chocolate.
- Children of Psychiatrists (The Last Psychiatrist). Do psychiatrists have crazier children? (See Dinah's post)
- Suicide risk in physicians. A European study (Hawton 2001) found that female doctors, and not male doctors, had increased suicide risk. Furthermore, specialties at highest risk included anesthesiology, generalists, and psychiatrists. A meta-analysis (Schernhammer 2004) found that physicians in general were 1.4 (men) and 2.3 (women) times more likely to commit suicide than the general population.
- Questions for us? Email at mythreeshrinksATgmailDOTcom. We'll answer some starting with Podcast #11.
Last week's musical snippet was from 1983 release, Genetic Engineering, from the Dazzle Ships album by Orchestral Manoeuvres in the Dark (OMD).
Find show notes with links at:
http://psychiatrist-blog.blogspot.com/2007/02/my-three-shrinks-podcast-10-be-mine.html
This podcast is available on iTunes (feel free to post a review). You can also listen to or download the .mp3 or the MPEG-4 file from mythreeshrinks.com. Thank you for listening.
technorati tags:psychiatry, psychiatrist, psychology, mental, health, medicine, podcast, psychiatric, chocolate, psychopharmacology, theobromine, caffeine, suicide, mood, depression, valentine, valentines
Blogged with Flock
Friday, February 09, 2007
Are You In Pain?
Or:
I Can't Think for Myself
Or:
One Great Way to Kill Trees
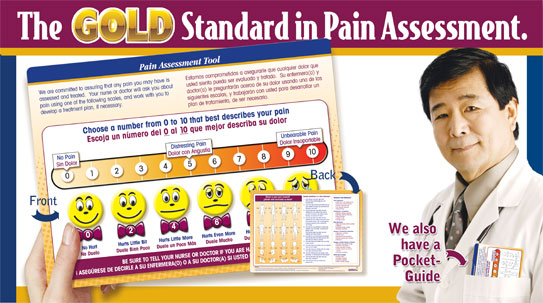
At the institution where I work, there is a requirement by JCAHO that all patients be assessed for pain. What this means, in practical terms, is that every patient at every visit in every department of the hospital is given a form and asked to mark off on a numerical scale how severe their pain is. For patients who can't negotiate that, there are smiley-to-frowny faces drawn and one can circle the face that best approximates one's degree of pain. Unlike the photo depicted above, my institution does not have the scale in color, and our smiley faces do not wear bow ties. You must sign the form at the bottom. I don't know what happens if you refuse, and the form is placed in your chart. We won't discuss what this does to the size of the charts, but hey, they pay me to be here.
I'm a psychiatrist, everyone who walks in the door, at least for the first time, is in pain. No No No No! Not that kind of pain, it has to be physical pain or it doesn't count! Does your body hurt? Now if the pain is more than a 3 out of 10, the patient is to be asked if they want to see a doctor. Oh, I am a doctor. 8 out of 9, maybe 9, It's that arthritis or maybe the chronic migraine. Yup, they have medicine for it. Okay, so now it's checked, they've seen the doctor, the sheet is signed, and it gets filed in the chart. Three cheers for us, we're JHACO compliant. Damn the trees, that's what Oregon's for.
So a patient comes to see me. The patient, John YoungGuy, is 27 years old. He has no significant medical or surgical history, he's here at the psychiatric clinic to get his mental illness treated. He's not in any physical pain (--He signed so it's a fact). The next week, Mr. YoungGuy returns to see me. I should ask him if he hurts? Why would he hurt? Wasn't I listening last week when he said he was healthy and had no pain. Really, he circled the zero and signed. Do I think he wouldn't tell me if he'd broken an arm on Saturday? By the fifth visit, by the fifth request to look at the demeaning smiley faces and sign off of that really, truly, he's not in any physical pain, might Mr. YoungGuy wonder if I'm not listening? If I'm not anything other than some idiot RobotShrink who sits there with a checklist (yup, I do, but at least a few of those questions are relevant, but trust me, the state-mandated 90 med check doesn't count if it isn't written up on the yellow sheet of paper).
I believe the intent of the mandate was good. Attention to pain, treatment of pain-- they are important things in medicine. The kneejerk phenomenon of signing off on a condescending smiley-face form, however, creates a culture where the goal is Compliance with regulatory agencies, not one of caring, attentiveness, creative solutions, or even of compassion. We shouldn't neglect pain, we (meaning all of us form-filler-outers from the orthopedist to the psychiatrist to the dermatologist) should enable relationships of trust and openness where the patient tells us they are in pain, and we address it as best we know how.
By the way: I lied. I never fill the forms out, they go straight into the trash, unchecked, unsigned. I feel way too foolish to even ask. Please don't tell anyone. You can, I hope, feel my pain.
--And by the way, has anyone seen Roy?
Thursday, February 08, 2007
Discover Your Inner Hero
 I have to admit I've never seen the television show Heroes. I understand the idea behind the show is that ordinary people discover they have extraordinary powers. That got me thinking about medical heroes. Usually when I hear that term I think about people like Dr. Edward Jenner who discovered the vaccination for small pox, or Walter Reed and his colleagues who voluntarily infected themselves with yellow fever to see if their vaccines worked. Medical heroes are people who do big, great things and cure diseases.
I have to admit I've never seen the television show Heroes. I understand the idea behind the show is that ordinary people discover they have extraordinary powers. That got me thinking about medical heroes. Usually when I hear that term I think about people like Dr. Edward Jenner who discovered the vaccination for small pox, or Walter Reed and his colleagues who voluntarily infected themselves with yellow fever to see if their vaccines worked. Medical heroes are people who do big, great things and cure diseases.I dunno, I'm more fond of the television Heroes' common-man definition. I like the ordinary anonymous docs who go out every day and do extraordinary things. I like the public psychiatrists.
I wish there were more of them. Of the six remaining state hospitals in Maryland, three have psychiatrist positions that have been standing vacant for months. I won't even mention how tough it is to find public psychiatrists to work in corrections.
It's not for lack of trying. In the 1970's our state created the Maryland Plan, a program sponsored jointly by the University of Maryland and the Maryland Department of Mental Hygiene to train and recruit psychiatry residents for employment in the public sector. The Maryland Plan was supposed to be a model program that would fill the physician recruitment needs of our state facilities. It hasn't, not even after closing one hospital.
So where are the doctors? There are 180 psychiatry residency programs in the country; Charm City has two of them and they turn out a dozen or so psychiatrists a year. One of the programs is within walking distance of my prison. They're not walking in my direction.
According to the U.S. Department of Health and Human Services health workforce analysis for Maryland:
"There were 1,093 psychiatrists, 5,390 psychologists and 8,000 social workers in Maryland in 2000. This was equal to 21.3 psychiatrists, 101.5 psychologists, and 150.6 social workers per 100,000 population. Maryland ranked 5th among states in psychiatrists per capita (emphasis mine), 1st among states in psychologists per capita, and 31st among states in social workers per capita."A search of the Maryland Psychiatric Society's directory will turn up 24 doctors under the category "public mental health system" but you'll get 192 if you search for "psychotherapy".
To add insult to injury, we can't even get public health service docs to work here because the Federal government has decided our need isn't great enough. To qualify for the loan repayment program psychiatrists have to work in a designated Health Professional Shortage Area (HPSA) with a need score of 19 or higher (on a scale of 0 to 100). The HPSA score is based on a convoluted algorithm involving poverty levels, demographic data and the number of mental health professionals in a given population. With a psychiatrist-to-resident ratio of 5000 to 1, Maryland doesn't even come close to the required 20,000 to 1 ratio needed to be a HPSA. There are no sites in Maryland with a need score this high. Correctional facilties get their own scoring system based on annual intakes and average length of stay, but again none of our facilities meet HPSA criteria even though we have longstanding open vacancies.
We're missing a few heroes. And they don't know what they're missing.
Wednesday, February 07, 2007
My Life As A Blogger

[posted by dinah]
This is the thing, while blogging is no longer ruining my life, and Shrink Rap is simply a blog, it continues to bring me satisfaction. I like having somewhere to come when something stirs me up. I like having an outlet to write -- I've said this before, but hey, repetition is part of the deal in psychotherapy, and while writing blog posts isn't "psychotherapy" it is therapeutic. One should take satisfaction and joy where one can find it, even if that means eating chocolate with friends while you talk about things you know nothing about, into some strange looking microphone that looks like something out of a sci fi movie and then you take pictures of your feet.
This is the other thing, I don't try to find topics to write about, I wait until I get hit by a wave of inspiration. The funny thing is, I seem to get hit by these inspiring waves at moments when I'm not near a computer. I'll get an idea. Then I'll get another idea. Then I'll get a third idea. Then when I'm near a computer, and either I can't get into the Dashboard (help, it's demanding I update to NEW blogger--Roy says not yet, and then he vanished under the floorboards) or my ideas have vanished.
So, I'm pleased I could get into the dashboard today. I'm sure what I wanted to say. I keep meaning to write about the importance of the relationship in psychotherapy, though I'm not sure what it is, exactly, that I want to say. That, you may have noticed, has never stopped me before. We're waiting on Roy for a 3 Blogger post on why we love psychiatry. I even linked it to a cute little poem. Roy hasn't finished yet, and I imagine he'll let me know when he has.
I've thought of asking if anyone one out there, say all those editors at Doubleday, wants to publish my latest novel? I'm a bit lost, though it's been mailed off to New York. I've been at it too long to let myself feel hopeful.
If you don't hear from us for a while, it's because I can't get in to post. I'm not sure how it happened today, yesterday I couldn't get access at all. Oh, and it didn't help that ClinkShrink had comcast problems.
Really just rambling. Thank you for listening.
Monday, February 05, 2007
ClinkShrink likes to hear about psychiatry from our readers in other countries. Lily (DrivingMissMolly) sent us a link to a blog owned by an Iraqi psychiatrist. Check out Psychiatry For All by Saminkie of Baghdad. The photos, the rendition of stigma in that country, the accounts of limited electricity and dealing with PTSD while the guns are still firing-- they are moving. I read the whole blog, it's not long, but it is a rich account of a poor and war-torn nation.
Sunday, February 04, 2007
My Three Shrinks Podcast 9: My Three Chromosomes
We decided to listen to Sophizo's suggestion and set up an email address for listeners to send questions to, and we will answer a couple in each podcast (starting with Podcast #11). We won't be able to answer them all, and we will not be able to answer any personal clinical questions. Send an email to mythreeshrinksATgmailDOTcom.
Also, feel free to go to iTunes and write a review (we had one, but it disappeared). We now have over 300 regular listeners (wow!), so maybe someone has something to say about us (maybe even something nice).
Last request: Dinah is only up to mid-season 2 in Lost, so she requests you post no spoilers for her on our blog, or she will be Positively Lost.
February 4, 2007:
Topics include:
- AJP: Genetics of depression. Two related articles in this month's Green Journal are from the GenRED study (Genetics of Recurrent Early-onset Major Depression). The Levinson article reports significant linkage for an area on chromosome 15 in 631 families with recurrent early-onset major depression ("early onset"=<40 yrs old). The Holmans article reports results of a genome scan in 656 families, finding significant linkage in areas of chromosomes 8, 15, and 17.
- Mandatory screening for depression? Clink conducts a thought exercise.
- Blogs & Identity. We talk about Dr. Anonymous' recent troubles after Fox News brands his one of 5 great medical blogs, and our feelings about blogging behind anonymous names (or not). See Dr A's post on the Myth of Anonymous Blogging. Moof's post is also worth reading on this topic. (We suspect his video blog may have given away his identity.) We look forwards to the congressional hearings on who leaked his identity and how high up this thing goes.
- Whither Public Psychiatry? Where have all the public sector psychiatrists gone? The number of HPSAs (Health Professional Shortage Areas) have decreased, while there seems to be less physician trainees who accept partial payment of their educational costs in return for a pledge to work in a HPSA after completing their training. But, Maryland has the most psychologists per capita in the US. (Search for Maryland psychiatrists at mdpsych.org.)
- Questions for us? Email at mythreeshrinksATgmailDOTcom. We'll answer some starting with Podcast #11 (in two weeks).
Next week: Biochemical effects of chocolate on mood (we really mean it this time). Also false positive drug tests, and children of psychiatrists.
Last week's musical snippet was from the 1986 release, Modigliani (Lost in Your Eyes), from their eponymous album by Book of Love [lyrics].
Find show notes with links at:
http://psychiatrist-blog.blogspot.com/2007/02/my-three-shrinks-podcast-9-my-three.html
This podcast is available on iTunes. You can also listen to or download the .mp3 or the MPEG-4 file from mythreeshrinks.com. Thank you for listening.
technorati tags:speed, genetics, depression, GenRED, chromosome, blogs, podcast, public, psychology, psychiatry, psychiatrist, AJP, article
Blogged with Flock
Saturday, February 03, 2007
Extra! Extra!

HELL FREEZES OVER
Dinah learns to use HTML.
BALTIMORE(AP)--Famed Shrink Rap blogger, Dinah, announced today that she successfully formatted her Blogger post with only minor HTML experience or assistance. She described her experience at an afternoon press conference:
"It was really easy," she said. "I just clicked the...whaddya call it? The link button. I clicked the link button."
[To appreciate the context of this post, please read the end of the comments on the previous post.]
Dinah, I want you to know I prepared this post last July. I've been hanging on to it for just this moment. Congratulations!
Thursday, February 01, 2007
Influenced by....
 If you recall, our dear ClinkShrink was recently ill with pneumonia and found herself the patient of a handsome young doc-in-the-box. She told us tales of her patienthood, and hid her doctor identity while the handsome young thing explained how the white blood count rises during an infection. Roy chimed in to say he also down-plays the doc thing when he's a patient: "I always heard that docs got worse care, not better. They don't get those nice explanations like you got, and the treating-doc tends to let the patient-doc drive the treatment plan bus more than is appropriate." I, on the other hand, can't stand relinquishing control, and could never lie low.
If you recall, our dear ClinkShrink was recently ill with pneumonia and found herself the patient of a handsome young doc-in-the-box. She told us tales of her patienthood, and hid her doctor identity while the handsome young thing explained how the white blood count rises during an infection. Roy chimed in to say he also down-plays the doc thing when he's a patient: "I always heard that docs got worse care, not better. They don't get those nice explanations like you got, and the treating-doc tends to let the patient-doc drive the treatment plan bus more than is appropriate." I, on the other hand, can't stand relinquishing control, and could never lie low.So, yesterday, I'm e-conversing with my wonderful friend, Linda, who is very sharp and very in tune to boundary issues. We got on the topic of something medical, and Linda e-mailed, "Countertransference, as you know, is a major issue in physicians treating physicians." She then steered me toward this sweet article by Jerome Groopman in the New Yorker, Medical Dispatches: What's The Trouble?
The article starts with a scenario starring Dr. Pat Croskerry, an ER doc who missed a diagnosis of cardiac disease in a slim, athletic, patient with no risk factors and a negative initial work-up. Dr. Croskerry assured the patient his chest pain wasn't cardiac, and oops, the patient bounced back later that day in the midst of an acute MI. Dr. Croskerry went on to study the cognitive factors which influence clinical decision making.
"But research shows that most physicians already have in mind two or three possible diagnoses within minutes of meeting a patient, and that they tend to develop their hunches from very incomplete information," Groopman writes. "The mistake that Croskerry made is called a “representativeness” error. Doctors make such errors when their thinking is overly influenced by what is typically true; they fail to consider possibilities that contradict their mental templates of a disease, and thus attribute symptoms to the wrong cause. "
Another type of error is deemed an 'availability' error: "Doctors can also make mistakes when their judgments about a patient are unconsciously influenced by the symptoms and illnesses of patients they have just seen." Ah, ClinkShrink didn't really have pneumonia, her doc-in-a-box missed the diagnosis of Multiple Personality Disorder because one of those clinky alters was coughing and the four prior patients had all had pneumonia! (Just kidding, there's only one ClinkShrink.)
Finally, Dr. Groopman goes on to talk about how doctors' feelings can get in the way of making the right diagnosis. He cites an example from his own practice, one where he missed finding an abscess in his favorite patient on the ward, a man he enjoyed discussing literature and running with.
"I was furious with myself. Because I liked Brad, I hadn’t wanted to add to his discomfort and had cut the examination short. Perhaps I hoped unconsciously that the cause of his fever was trivial and that I would not find evidence of an infection on his body. This tendency to make decisions based on what we wish were true is what Croskerry calls an “affective error.” Groopman goes on to write, "When people are confronted with uncertainty—the situation of every doctor attempting to diagnose a patient—they are susceptible to unconscious emotions and personal biases, and are more likely to make cognitive errors."
I suppose I wanted there to be a story about a doctor missing the diagnosis on another doctor, it is, afterall, what I was thinking about. This will be good enough, though. Our relationships with our patients-- perhaps even more so in psychiatry-- are complicated. Our feelings, our hopes, our own issues-- maybe they get in the way, certainly they add to the mix.
Post Script: Check out The Last Psychiatrist, post of 1/31/07: When the Patient's Parent is a Psychiatrist and a Patient and You Just Want to Go To Bed.
Subscribe to:
Posts (Atom)